![]()
CME: WPW & AF Case Report
Here are the ECG’s that we discussed at the CME Quiz
Presenting ECG


This shows the rhythm is irregularly irregular with no perceivable P waves = Atrial Fibrillation. The QRS complex appears abnormal, slightly broad with slurring of the initial portion of the complex (note that this is similar morphology with the post-cardioversion QRS complex) – suggestive of a pre-excitation syndrome. So this likely represents atrial fibrillation in a person with an accessory pathway passing through the AV Node (Orthodromic). Blocking of the AV node in this situation may push the atrial depolarisations at >300beats per minute down the accessory pathway rather than the AV node. The AV node has an inbuilt delay that protects the ventricles from exposure to the full rate of atrial depolarisations and the potential of precipitating VF (better explained by Amal Mattu below). Hence, this patient was electrically cardioverted, rather than using AV nodal blocking drugs (metoprolol, verapamil, adenosine etc…), with the post-cardioversion ECG below.
Post-cardioversion ECG
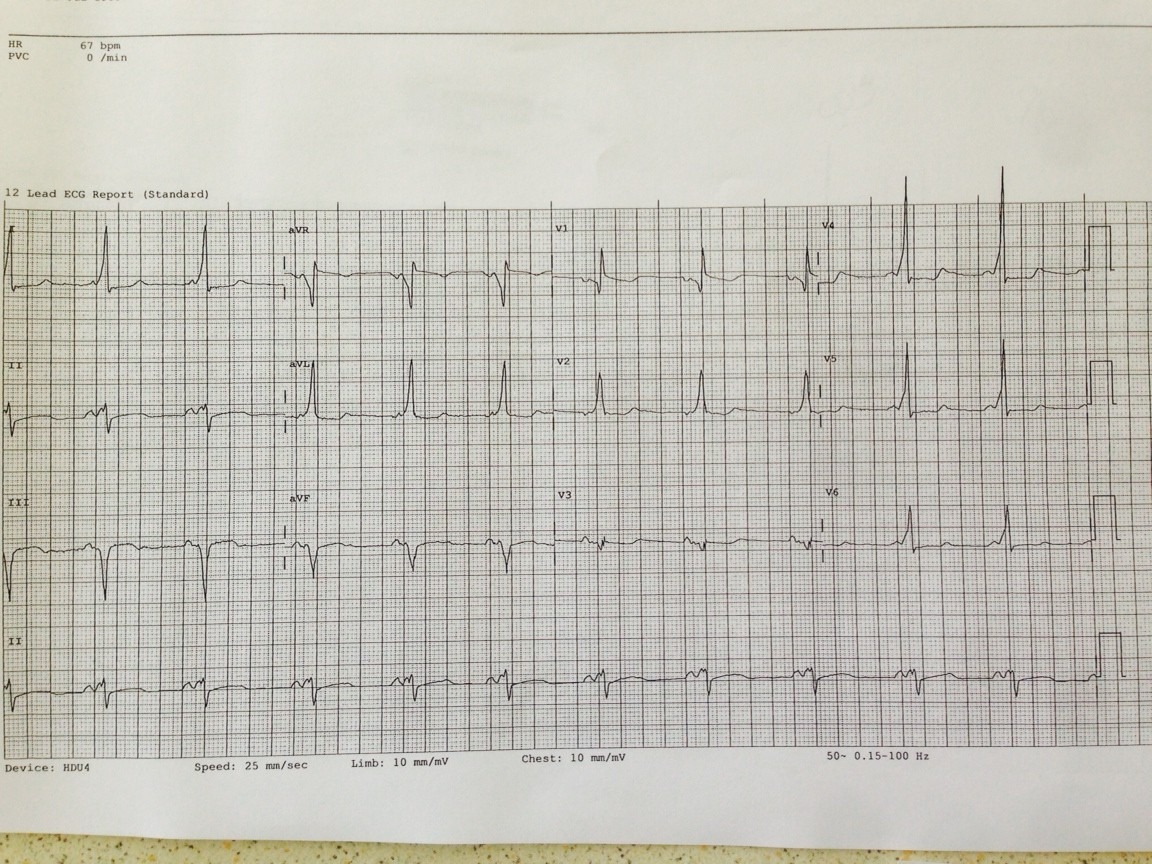{kind=link}
Here are some links to some great summaries on WPW:
- Pre-Excitation Syndromes by John Larkin
- Here is another interesting case discussion (courtesy of Deanne) titled “Puzzling Paroxysmal Palpitations” by Ed Burns from LITFL that discusses the differential for a Regular Broad Complex Tachycardia
